Looking at the full scope of PAD: Cases, techniques, and economic considerations for complex disease.
Current Challenges for the Modern Management of PAD
An overview of contemporary and emerging practices in peripheral artery disease.
BY FANNY S. ALIE-CUSSON, MD, AND JEAN M. PANNETON, MD, FRCSC, FACS
Peripheral artery disease (PAD) affects an increasingly high number of patients across the globe. Unfortunately, as our population ages, the incidence of PAD also increases and the burden of cardiovascular disease on health care costs is heavier than ever before. Luckily, the field of vascular intervention is in full effervescence with countless new devices and technologies emerging onto the market, further diversifying the available armamentarium to address this chronic and incurable condition.
PAD is a heterogenous disease process that affects patient groups differently; for example, younger patients and those who smoke typically present with inflow disease at the aortoiliac and femoropopliteal levels, whereas older or diabetic patients generally present with distal outflow disease at the tibioperoneal level. Symptomatology varies broadly from intermittent claudication (IC) to tissue loss, and the corresponding disease management also varies greatly. A generally accepted concept is that asymptomatic disease does not warrant intervention, and instead, optimal medical management should represent the mainstay of treatment for these patients. IC should be intervened upon when it is severe or refractory to conservative treatment. When indicated, determining the timing of intervention and navigating the wide array of therapeutic options present a great challenge for modern vascular specialists.
Multiple approaches, algorithms, and rationales to therapy have been proposed. The elderly comorbid patient with a short life expectancy has traditionally been the preferred endovascular patient, but indications for endovascular treatment are steadily becoming broader. The decision-making process in choosing between open or endovascular therapy is not clearly established and varies widely between practitioners and practice settings. Additionally, therapeutic approaches should be dictated by therapy goals, whether it be improvement of walking distance or resolution of rest pain and wound healing. Refractory IC is generally addressed via an endovascular approach first, with operative management reserved for more severe symptomatology. An important question should be answered by the long-awaited BEST-CLI trial.1 Hopefully, BEST-CLI will further define the optimal management algorithm for infrainguinal occlusive disease and allow for a more tailored therapeutic approach for patients with critical limb ischemia.
Iliac Disease

Figure 1. Aortoiliac angiogram showing severe calcified bilateral common iliac artery ostial stenoses.
Endovascular treatment of inflow disease has been increasingly successful over the years and skilled practitioners are now tackling the most complex iliac lesions. The GORE® VIABAHN® VBX Balloon Expandable Endoprosthesis (VBX Stent Graft) offers excellent primary patency rates in challenging aortoiliac occlusive lesions. In the VBX FLEX study, 32.1% of patients presented with TransAtlantic Inter-Society Consensus Classification II (TASC II) C/D lesions, and 42.5% of patients received kissing stents at the aortic bifurcation. The primary patency rate was 96.9% at 9 months with no significant difference in patency rates between TASC II A/B versus C/D lesions.2 Figures 1 through 3 demonstrate the use of kissing VBX Stent Grafts for severe stenosis of both common iliac arteries at their origin with excellent angiographic results. These covered stents represent a safe option in managing high-grade, severely calcified or excentric lesions with an inherently higher risk of complications from recanalization as they allow for simultaneous management of dissections and potential ruptures.
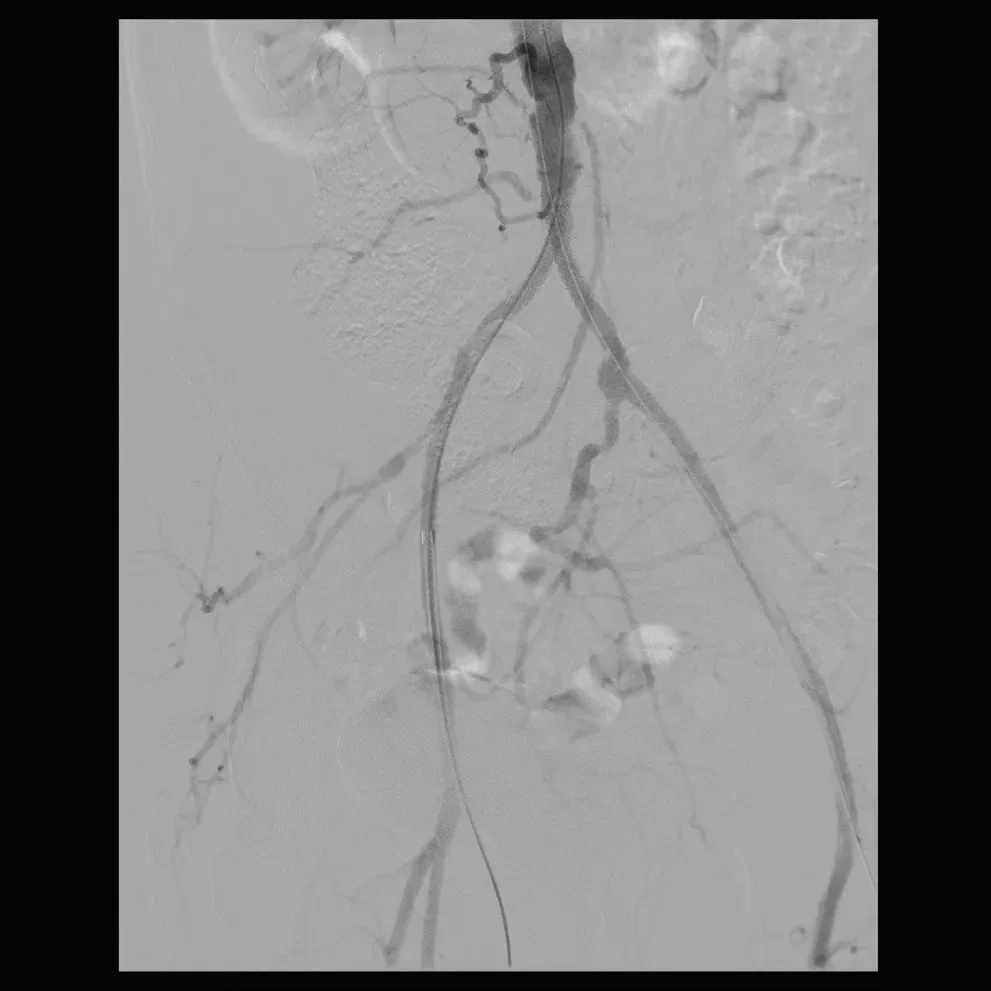
Figure 3. Excellent results can be seen on completion angiogram.
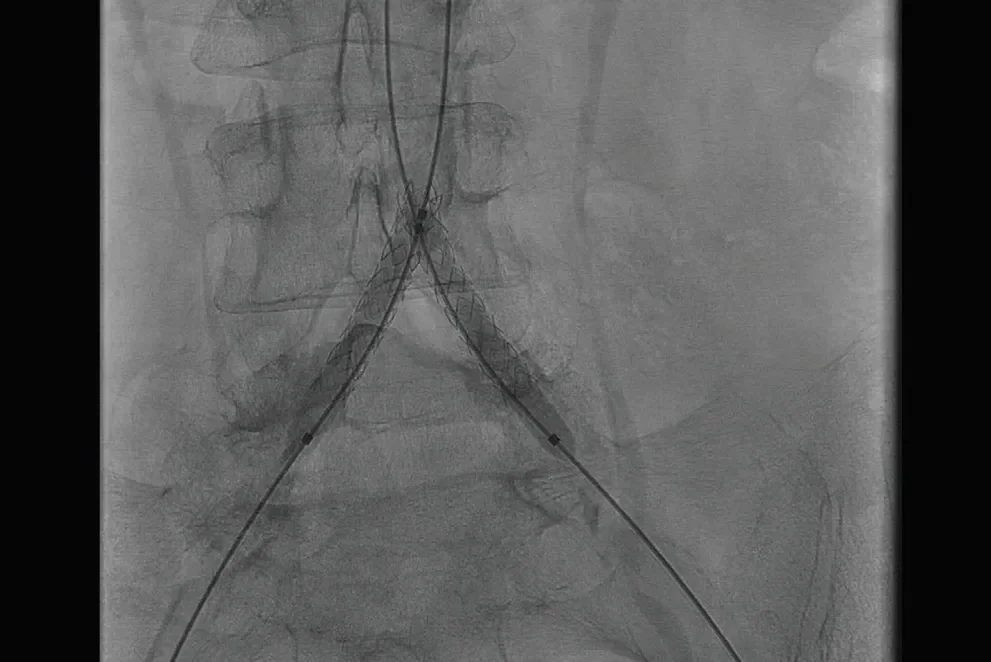
Figure 2. Deployment of bilateral common iliac artery GORE® VIABAHN® VBX Balloon Expandable Endoprosthesis kissing covered stents.
Femoropopliteal Disease
Treatment for femoropopliteal disease is now steering away from the full-metal jacket era. Instead, a more comprehensive strategy to minimize stent complications while optimizing patency rates is employed with an As Low As Reasonably Achievable (ALARA) strategy. The body of clinical evidence supporting the use of the GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface for treating long lesions (> 10–15 cm) and chronic occlusions of the femoropopliteal segment continues to grow. The most recent study to evaluate the GORE VIABAHN Endoprosthesis performance in the superficial femoral artery demonstrated a 12-month primary patency of 88% in lesions with an average length of 22 cm.3 There are now five multicenter, prospective, randomized, or single-arm studies that have evaluated the heparin-coated GORE VIABAHN Endoprosthesis demonstrating an average 12-month primary patency of 75% in long (average lesion length, 22 cm), complex (n = 302 chronic total occlusions out of 422 limbs) lesions.3-7 Data from the RELINE clinical trial support the use of the GORE VIABAHN Endoprosthesis for the treatment of in-stent restenosis (ISR) with a 75% primary patency rate and 80% freedom from target lesion revascularization (TLR) at 12 months with a mean treated lesion length of 17.3 cm. In comparison, percutaneous transluminal angioplasty (PTA) was associated with a 28% primary patency rate and 42% freedom from TLR at 12 months.8 However, edge restenosis, potential for acute limb ischemia by covering critical collateral branches, and stent thrombosis are caveats that need to be considered. Complete coverage of all diseased portions of the stented artery and avoiding oversizing of stent grafts may improve outcomes.
The popliteal artery is more difficult to address via endovascular approaches given its location and the dynamic stresses to which it is exposed. Therefore, stent placement in this arterial segment is particularly prone to fracture due to insufficient flexibility and heightened breakability, inevitably leading to secondary complications. New generations of nitinol stents, such as the GORE® TIGRIS® Vascular Stent, are designed to adapt to the ever-changing anatomy of the distal artery with a higher resistance to fracture via an interconnecting heparinbonded polymer mesh. Primary patency at 12 months was 81.5%.9 More recent data have also shown its efficacy in combination with a GORE VIABAHN Endoprosthesis.10
Despite the ALARA strategy rationale, residual stenosis or dissection following PTA remain accepted indications for stent placement. Technology has fortunately evolved from standard laser-cut nitinol stents and their high fracture rates to more conformable interwoven nitinol stents, which are associated with better patency rates as well as a reduced incidence of stent fractures. Despite this, ISR unfortunately represents one of the toughest challenges we face as endovascular practitioners. Multiple trials have supported the use of drug-coated balloons to improve patency rates in management of ISR, such as the FAIR trial,11 with freedom from TLR rates of 96.4% with the MEDTRONIC IN.PACT Admiral Drug-Coated Balloon versus 81% with plain old balloon angioplasty (P = .0117) at 6 months and 90.8% versus 52.6% (P < .0001) at 12 months, respectively. The DEBATE-ISR trial showed similar results but, unfortunately, the difference did not persist at the 3-year mark.12 Atherectomy devices, such as the SPECTRANETICS® EXCIMER Laser System, were also introduced as a potential solution to treat ISR by debulking the intimal hyperplastic tissue, thus improving luminal gain.13
Surgical bypass procedures still have an important role in certain instances, namely in younger patients with aortoiliac disease, long-segment femoropopliteal disease, severe tibial disease, or failed prior endovascular therapy. Autologous vein grafts are preferable, but another option would be expanded polytetrafluoroethylene (ePTFE) synthetic bypass grafts. Notably, the GORE® PROPATEN® Vascular Graft has been shown to offer promising results in infrainguinal bypass compared with standard ePTFE, with 74.5% overall primary patency at 5 years versus 56.2% for standard ePTFE grafts (P = .03).14
Conclusion
Modern endovascular technology is rapidly evolving, and outcomes are steadily improving. However, as we look ahead, multiple challenges remain, such as minimizing neointimal hyperplasia, refining our approach to tibioperoneal interventions, and managing ISR more effectively.
This supplement offers an up-to-date overview of the interventional management of complex PAD with a heavier focus on endovascular approaches. We hope to allow readers to have a better grasp on current available technologies and their evidence-based indications.
- Menard MT, Farber A, Assmann SF, et al. Design and rationale of the best endovascular versus best surgical therapy for patients with critical limb ischemia (BEST-CLI) trial. J Am Heart Assoc. 2016;5:e003219.
- Bismuth J, Gray BH, Holden A, et al. Pivotal study of a next-generation balloon-expandable stent-graft for treatment iliac occlusive disease. J Endovasc Ther. 2017;24:629-637.
- Ohki T, Kichikawa K, Yokoi H, et al. Outcomes of the Japanese multicenter Viabahn trial of endovascular stent grafting for superficial femoral artery lesions. J Vasc Surg. 2017;66:130-142.e1.
- Lammer J, Zeller T, Hausegger KA, et al. Sustained benefit at 2 years for covered stents versus bare-metal stents in long SFA lesions: the VIASTAR Trial. Cardiovasc Interv Radiol. 2015;38:25-32.
- Zeller T, Peeters P, Bosiers M, et al. Heparin-bonded stent-graft for the treatment of TASC II C and D femoropopliteal lesions: the Viabahn-25 cm Trial. J Endovasc Ther. 2014;21:765-774.
- Reijnen M, van Walraven L, Fritschy W, et al. 1-year results of a multicenter, randomized controlled trial comparing heparin-bonded endoluminal to femoropopliteal bypass. J Cardiovasc Interv. 2017;10:2320-2331.
- Saxon RR, Chervu A, Jones PA, et al. Heparin bonded, expanded polytetrafluoroethylene lined stent graft in the treatment of femoropopliteal artery disease: 1 year results of the VIPER (Viabahn Endoprosthesis with Heparin Bioactive Surface in the Treatment of Superficial Femoral Artery Obstructive Disease) Trial. J Vasc Interv Radiol. 2013;24:165-173.
- Bosiers M, Deloose K, Callaert J, et al. Superiority of stent-grafts for in-stent restenosis in the superficial femoral artery: twelve-month results from a multicenter randomized trial. J Endovasc Ther. 2015;22:1-10.
- Sibé M, Kaladji A, Boirat C, et al. French multicenter experience with GORE TIGRIS Vascular Stent in superficial femoral and popliteal arteries. J Vasc Surg. 2017;65:1329-1335.
- Lucatelli P, Cini M, Tommasino G, et al. Use of the Gore Tigris vascular stent in advanced femoropopliteal peripheral arterial disease. J Vasc Interv Radiol. 2017; 29:614-622.
- Krankenberg H, Tübler T, Ingwersen M, et al. Drug-coated balloon versus standard balloon for superficial femoral artery in-stent restenosis: the randomized femoral artery in-stent restenosis (FAIR) trial. Circulation. 2015;132:2230‑2236.
- Grotti S, Liistro F, Angioli P, et al. Paclitaxel-eluting balloon vs standard angioplasty to reduce restenosis in diabetic patients with in-stent restenosis of the superficial femoral and proximal popliteal arteries: three-year results of the DEBATE-ISR study. J Endovasc Ther. 2016;23:52-57.
- Dippel EJ, Makam P, Kovach R, et al. Randomized controlled study of Excimer laser atherectomy for treatment of femoropopliteal in-stent restenosis: initial results from the EXCITE ISR trial (EXCImer Laser Randomized Controlled Study for Treatment of FemoropopliTEal In-Stent Restenosis). JACC Cardiovasc Interv. 2015;8:92-101.
- Samson RH, Morales R, Showalter DP, et al. Heparin-bonded expanded polytetrafluoroethylene femoropopliteal bypass grafts outperform expanded polytetrafluoroethylene grafts without heparin in a long-term comparison. J Vasc Surg. 2016;64:638-647.


Proven across a broad range of complex cases, the versatility of the GORE® VIABAHN® Endoprosthesis with PROPATEN Bioactive Surface* enables you to deliver high patency and durable outcomes to minimize interventions for your patients.

Addressing the problem of thrombus formation on the luminal surface of a vascular graft is a challenge faced by all vascular surgeons. The GORE® PROPATEN® Vascular Graft is specifically designed for those vascular procedures in which the risk of acute graft thrombotic failure is of clinical concern.
Endovascular Today February 2019 Supplement
Looking at the Full Scope of PAD
Fanny S. Alie-Cusson, MD
Fellow
Division of Vascular Surgery
Eastern Virginia Medical School
Norfolk, Virginia
Disclosures: None.
Jean M. Panneton, MD, FRCSC, FACS
Professor of Surgery
Chief and Program Director
Division of Vascular Surgery
Eastern Virginia Medical School
Norfolk, Virginia
Disclosures: Consultant to Gore & Associates, research investigator, and honorary speaker.