Treating symptoms of portal hypertension
Many of the treatments for portal hypertension focus on managing symptoms. For patients who have cirrhosis and complications of portal hypertension, medication, lifestyle modifications and a specialized diet may be used to help manage the condition. For diet modification, a low salt or restricted protein diet may be recommended and patients may be referred to a dietician for advice on what foods to avoid, including alcohol avoidance.
Paracentesis, endoscopic band ligation (EBL) and TIPS may also be a part of your treatment.
Treating Ascites
Diuretics are often prescribed to reduce fluid retention. Sometimes medication alone is not sufficient, or a patient cannot tolerate diuretics. In these situations, large-volume paracenteses (LVP) may be needed to treat the ascites. LVP involves using an ultrasound-guided needle to drain the abdomen of fluid buildup. The fluid removed will be examined for signs of infection and to help determine if the fluid is caused by portal hypertension.
Some patients with portal hypertension develop refractory ascites, where ascites does not respond to diuretics or recurs shortly after LVP. Patients with refractory ascites typically require frequent paracentesis procedures. Based on current guidelines, if you have refractory ascites you should discuss being evaluated for a TIPS procedure with your doctor.1
Risks associated with LVP
In general, the development of ascites indicates advanced liver disease and patients may be referred for a liver transplant. Even in those circumstances, LVP may continue while waiting for a transplant. LVP can be costly,2 time consuming and may be accompanied with one or more risks.
Potential risks associated with LVP can include, but are not limited to3-6:
- Leaking of fluid at insertion site
- Bleeding at insertion site and internally
- Infection
- Electrolyte imbalance
- Bowel perforation
- Paracentesis-induced circulatory dysfunction
- Kidney injury
Treating variceal bleeding
Variceal bleeding is one of the most significant complications of varices resulting from portal hypertension. Varices are enlarged veins, often around the stomach and esophagus, and can be treated in a number of ways. Currently, the two most widely used treatments to prevent and treat esophageal variceal bleeding are medication (non-selective beta-blockers [NSBB]) and a minimally invasive procedure called variceal band ligation (VBL) or EBL. It is common that EBL is repeated when bleeding episodes recur. Gastric varices are located on the stomach, and are often considered a medical emergency when they bleed. Patients with gastric variceal bleeding are often treated with intravenous antibiotics, vasoactive medications and may undergo a minimally invasive procedure where a glue or tissue adhesive is injected at the site of the bleed. If those measures are unable to stop the bleeding, rescue measures, such as balloon tamponade, balloon-occluded retrograde transvenous obliteration (BRTO), TIPS or surgery may be required.
Risks associated with variceal bleeding
Every episode of variceal bleeding increases the patient's risk of morbidity and mortality. Complications of variceal bleeding may be due to the bleeding episode itself or related to procedures used to treat bleeding episodes. These complications may include, but are not limited to7-9:
- Infection
- Hypotension and circulatory shock
- Hepatic encephalopathy
- Aspiration pneumonia
- Ulcers
- Esophageal perforation
- Death
The treatments to prevent bleeding are themselves not without risk. Although rare, adverse events from EBL can include perforation of the esophagus and ulcer-related bleeding.10 Beta blocker medications, often prescribed to help lower blood pressure, can cause side-effects like fatigue, sexual dysfunction, weight gain, shortness of breath, low blood pressure and nausea. If you are experiencing recurrent bleeding episodes and require multiple EBL procedures, ask your doctor if you are a good candidate for a TIPS procedure.
TIPS procedure for treating portal hypertension
If other treatments for ascites or variceal bleeding are not effective, then your doctor may recommend a TIPS procedure as an appropriate therapy. While EBL and LVP treat the complications of portal hypertension, TIPS reduces portal hypertension, which is the underlying cause of the complications. Recent clinical evidence shows that many patients with portal hypertension experience higher survival and freedom from complications by undergoing TIPS earlier.11
But what is a TIPS procedure? A TIPS procedure creates a new channel to route blood flow through the damaged liver and into the main blood vessels that lead blood back to the heart. A TIPS stent placed inside this channel allows a portion of blood to bypass the liver, reducing portal hypertension and its complications.12
The TIPS procedure is a minimally invasive procedure, typically requiring a short hospitalization. TIPS reduces portal hypertension, so alternative treatments such as medications, paracentesis for ascites and the treatment of varices may be needed less frequently or not at all. Ask your doctor if you are a candidate for an early TIPS procedure.
What to expect during the TIPS procedure
Your physician may have specific medical guidance on what to expect when having a TIPS procedure. Generally, the procedure is performed in a hospital under sedation or general anesthesia by specially trained doctors called interventional radiologists. The procedure typically takes two to three hours, but may take longer. Your doctor will give you direction about limiting food intake and medications before your procedure. During the TIPS procedure, you will be connected to monitors to track heart rate and blood pressure and an intravenous line to administer medications.
The doctor uses X-ray pictures and X-ray dye (also called contrast dye) to guide the procedure. A needle is guided through the introducer sheath to the hepatic vein. Using X-ray guidance, the needle is directed from the hepatic vein into the portal vein, creating a tunnel between the hepatic and portal veins. A special balloon is used to enlarge the liver tunnel, and the doctor inserts the TIPS stent into the tunnel to help it remain open and allow blood flow (see Figure 1).
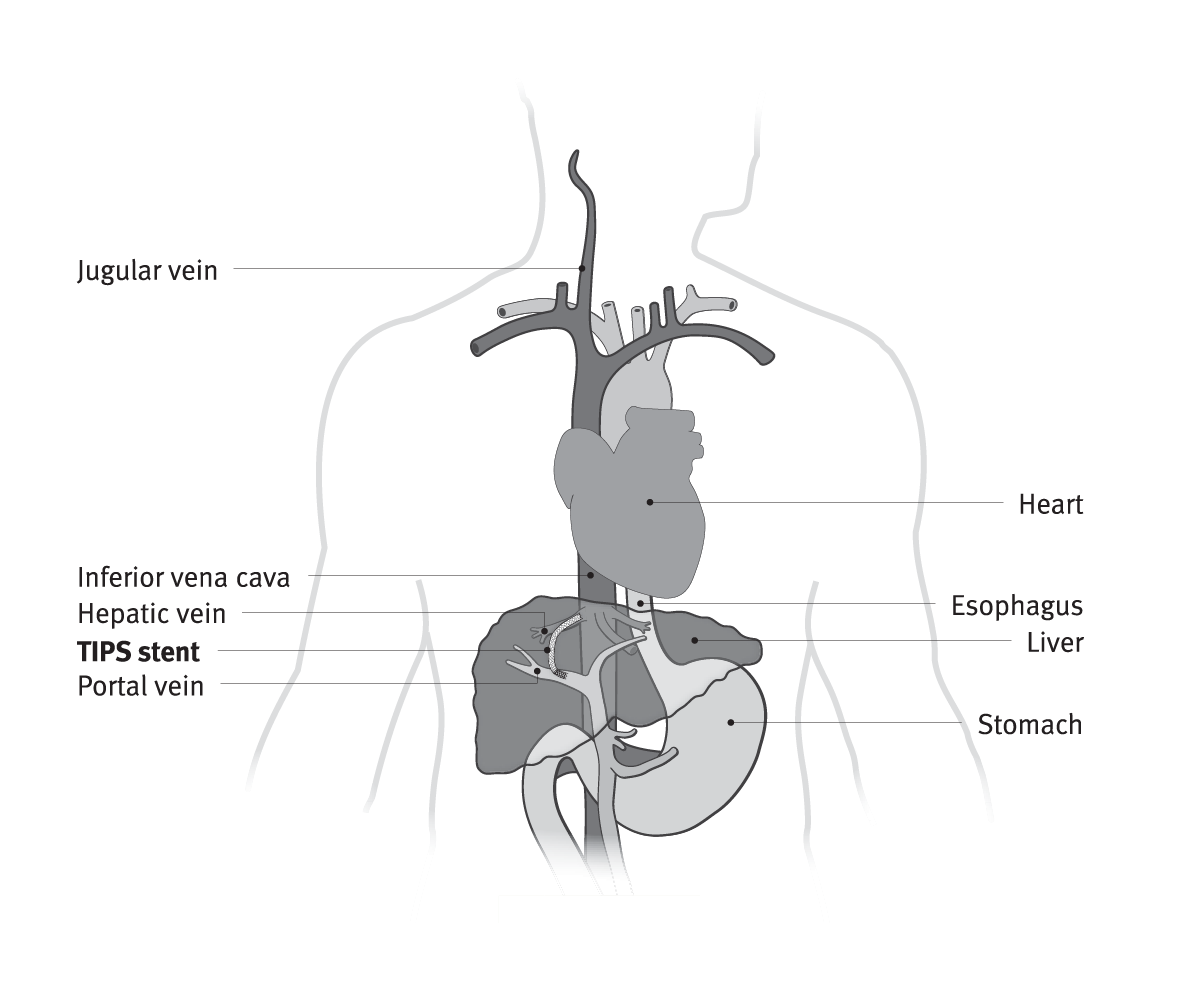
Figure 1.
What to expect following a TIPS procedure
The TIPS procedure typically requires a hospital stay of one or more days, but could be longer.12 During your hospital stay, your doctor will monitor your health and may conduct additional tests. Once home, a specialized diet may be suggested and medications may be prescribed to manage your treatment. Contact your doctor immediately if you experience disorientation or confusion. It is important to follow your physician’s recommendation for monitoring the TIPS stent and your health. Often a series of post-procedure check-ups will be scheduled at one month and six months and your doctor may recommend additional check-ups. The follow-up exams may consist of routine X-rays, an ultrasound and blood tests.
It is advisable to have a good support system available to participate in your post-TIPS care to help with diet, medication, doctor’s appointments and to generally monitor your condition for any warning signs.
Are there any risks associated with TIPS ?
All surgical procedures have risks. Some potential risks associated with a TIPS procedure can include, but are not limited to13:
- Fever
- Stiffness, bruising or soreness in the neck
- Reactions to medicines or dye
- Hepatic encephalopathy
- Damage to blood vessels
- Heart problems or abnormal heart rhythms
- Infection
Recent studies11,14-16 indicate that for some patients, there is no increase of hepatic encephalopathy with TIPS when compared to standard treatments.
There may be additional risks that are not mentioned here. Speak with your doctor about any concerns or risks, complications you experience, and proper post-procedure treatment. If you experience a worsening of symptoms, contact your doctor.
The information provided is intended to be general guidance based on current medical practices in the field. The steps described here may not be complete, and are not intended to be a replacement for the Instructions for Use or the education, training and professional judgment of healthcare providers (HCP). Licensed HCPs remain responsible for making decisions about patient care and the use of medical technologies.
This information is intended for education and awareness only. Patients should consult their physician for information on the risks associated with the devices and surgical procedures discussed in this website. All surgical procedures carry potential health risks. Not all patients will be candidates for treatment with these devices, and individual outcomes may vary.
Always follow physician advice on your post-surgery care and recovery.
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. Journal of Hepatology 2018;69(2):406-460.
- Kwan SW, Allison SK, Gold LS, Shin DS. Cost-effectiveness of transjugular intrahepatic portosystemic shunt versus large-volume paracentesis in refractory ascites: results of a Markov model incorporating individual patient-level meta-analysis and nationally representative cost data. Journal of Vascular & Interventional Radiology 2018;29(12):1705-1712.
- De Gottardi A, Thévenot T, Spahr L, et al. Risk of complications after abdominal paracentesis in cirrhotic patients: a prospective study. Clinical Gastroenterology & Hepatology 2009;7(8):906-909. https://www.cghjournal.org/article/S1542-3565(09)00438-8/fulltext
- Shlamovitz GZ, Shah NR. Paracentesis technique. Medscape website. Updated: Apr 06, 2020. Accessed September 18, 2020. https://emedicine.medscape.com/article/80944-technique#c3
- Berseth CL. Physiologic and inflammatory abnormalities of the gastrointestinal tract. In: Taeusch HW, Ballard RA, Gleason CA, eds. Avery's Diseases of the Newborn. 8th ed. Philadelphia, PA: Elsevier Saunders; 2005;72:1103-1112. https://www.sciencedirect.com/topics/medicine-and-dentistry/paracentesis
- Lindsay AJ, Burton J, Ray CE Jr. Paracentesis-induced circulatory dysfunction: a primer for the interventional radiologist. Seminars in Interventional Radiology 2014;31(3):276-278. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4140947/
- McKay R, Webster NR. Variceal bleeding. Continuing Education in Anaesthesia Critical Care & Pain 2007;7(6):191-194. https://doi.org/10.1093/bjaceaccp/mkm038
- Endoscopic treatment for variceal bleeding caused by cirrhosis. UW Health website. Updated: April 15, 2020. Accessed September 18, 2020. https://www.uwhealth.org/health/topic/special/endoscopic-treatment-for-variceal-bleeding-caused-by-cirrhosis/aa87512.html#aa87512-sec
- Cesario KB, Choure A, Modha K, Carey WD. Variceal hemorrhage. The Cleveland Clinic Foundation website. Published April 2013. Accessed September 18, 2020. http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/hepatology/variceal-hemorrhage/
- Karadsheh Z, Allison H. Primary prevention of variceal bleeding: pharmacological therapy versus endoscopic banding. North American Journal of Medical Sciences 2013;5(10):573-579. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3842697/
- Hernández-Gea V, Procopet B, Giráldez Á, et al: International Variceal Bleeding Observational Study Group and Baveno Cooperation. Preemptive-TIPS improves outcome in high-risk variceal bleeding: an observational study. Hepatology 2019;69(1):282-293. https://aasldpubs.onlinelibrary.wiley.com/doi/full/10.1002/hep.30182
- Transjugular Intrahepatic Portosystemic Shunt (TIPS). RadiologyInfo.org For Patients website. Published March 05, 2019. Accessed November 10, 2020. https://www.radiologyinfo.org/en/info.cfm?pg=tips
- A.D.A.M. Medical Encyclopedia [Internet]. Johns Creek (GA): Ebix, Inc., A.D.A.M.; c1997-2020. Transjugular intrahepatic portosystemic shunt (TIPS); [updated 2020 Sept 16; reviewed 2019 Jan 4; cited 2020 Sept 18];[about 2 p]. Available from: https://medlineplus.gov/ency/article/007210.htm
- García-Pagán JC, Caca K, Bureau K, et al. Early TIPS (Transjugular Intrahepatic Portosystemic Shunt) Cooperative Study Group. Early use of TIPS in patients with cirrhosis and variceal bleeding. New England Journal of Medicine 2010;362(25):2370-2379. https://www.nejm.org/doi/full/10.1056/NEJMoa0910102
- Garcia-Pagán JC, Di Pascoli M, Caca K, et al. Use of early-TIPS for high-risk variceal bleeding. Results of a post-RCT surveillance study. Journal of Hepatology 2013;58(1):45-50.
- Bureau C, Thabut D, Oberti D, et al. Transjugular intrahepatic portosystemic shunts with covered stents increase transplant-free survival of patients with cirrhosis and recurrent ascites. Gastroenterology 2017;152(1):157-163. http://www.sciencedirect.com/science/article/pii/S0016508516351101

Refer to Instructions for Use at eifu.goremedical.com for a complete description of all applicable indications, warnings, precautions and contraindications for the markets where this product is available. RXOnly
INDICATIONS FOR USE IN THE U.S: The GORE® VIATORR® TIPS Endoprosthesis is indicated for use in the de novo and revision treatment of portal hypertension and its complications such as variceal bleeding, gastropathy, refractory ascites, and/or hepatic hydrothorax.